Always a pleasure to listen to J.Wolchok- Some history on immune therapy- IL2 approved in 1995 and already showed the 'tail' of the immune therapies that we like to see so much. Unfortunately not for many patients and coming with considerable toxicity.

'Pseudoprogression'- tumours seem to grow but are in effect infiltrated by immune cells. For that reason, immune RECIST were developed to distinguish progression from something that looks like progression but in reality is a response by the immune system.
Long-term survival on Ipi- 20%
from Schadendorf et al. 2015

the full publication is available here.
PDL1 as biomarker
as rather not as Wolchok was very vocal on PDL1 NOT being suitable to make treatment decisions whether to give an anti-PD1 antibody (Keytruda, Opdivo) or not. Even patients without PDL1 expression can respond to anti-PD1 antibodies and PDL1 is not a stable biomarker- it can be induced and change over time.
This is besides the fact that tests for PDL1 are not consistent, so different tests on the same tissue sample will not give the same results!
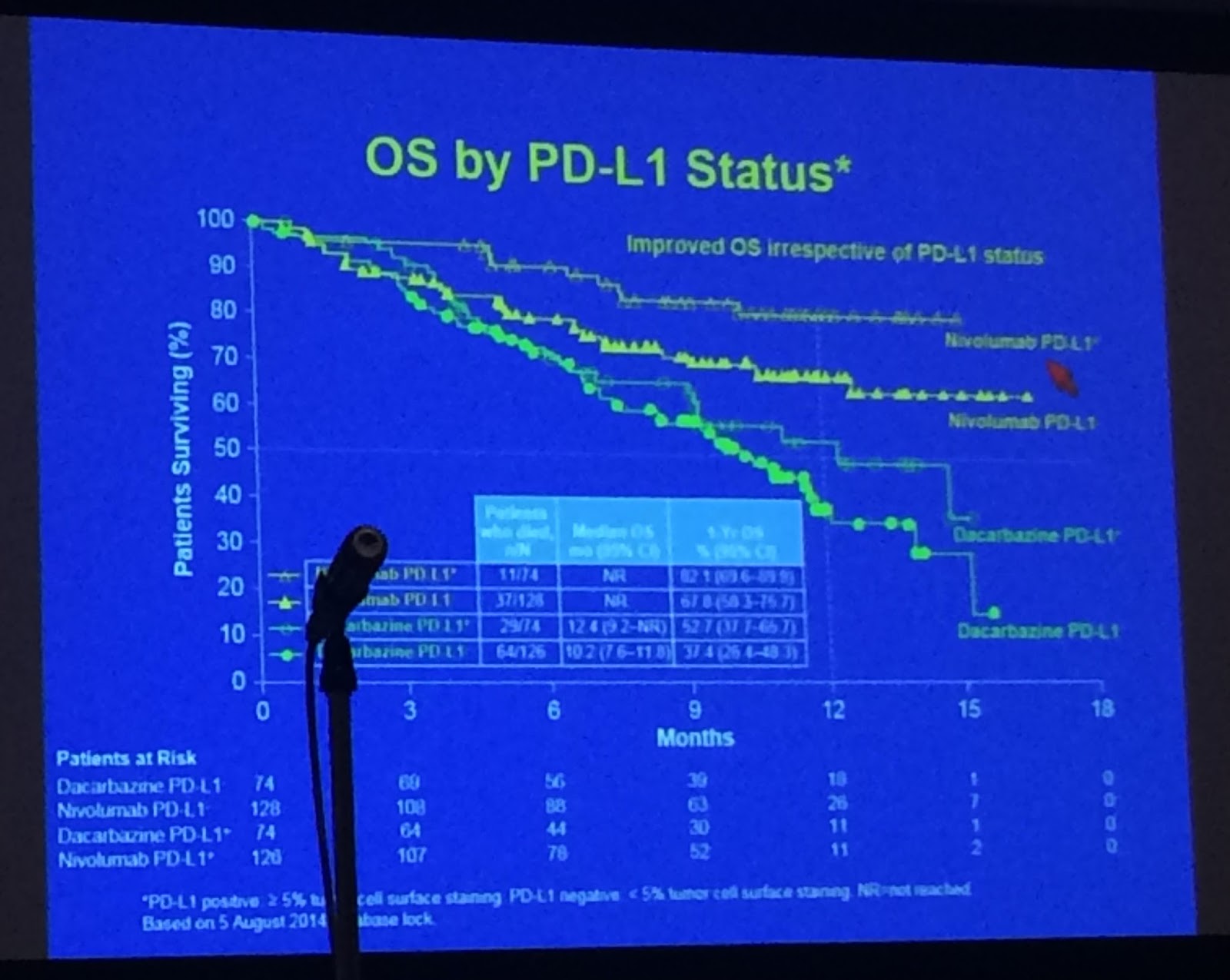
Hard to see but top curve is overall survival for patients whose tumours were PDL positive, the next lower one patients whose tumours who are PDL1 negative- and then come the DTIC ones..... which should have never been there in the first place!!
Combination of IPI plus PD1
Very interesting point on IPI plus PD1 given together or after each other- it appears that the concentration of how much Ipi is present in the blood matters: patients with more Ipi left do better.

67.5% of patients 81/120 who discontinued Nivo + Ipi due to side effects developed a response.
No comments:
Post a Comment